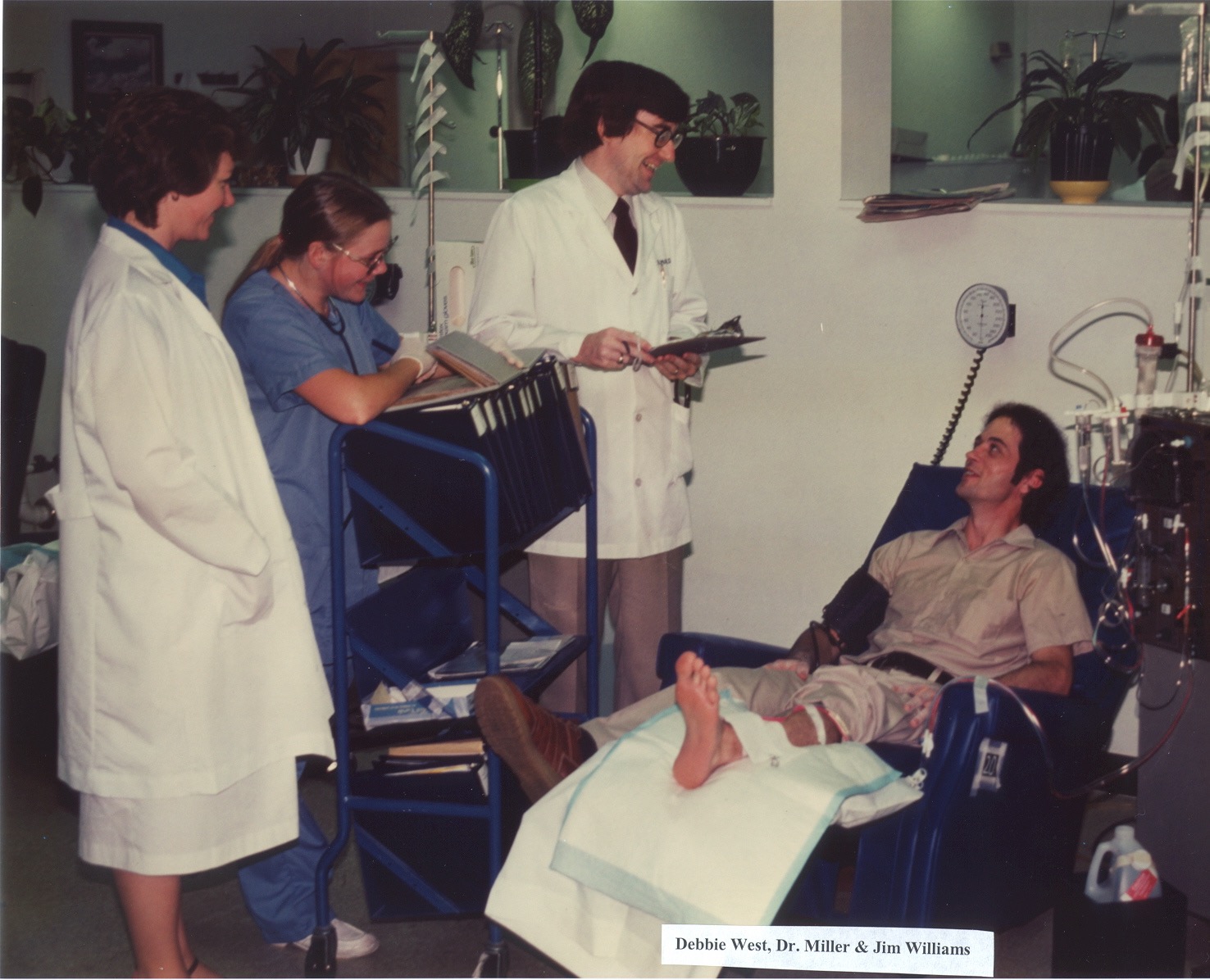
DCI was founded in 1971 in Nashville, Tenn., as a not-for-profit dialysis provider by nephrologist Dr. H. Keith Johnson. At that time, there was no Medicare funding for dialysis, and most patients did not have insurance coverage for dialysis. This meant that many patients couldn’t afford treatment and would face the difficult choice of mortgaging their homes, selling their farms, spending their children’s college funds, or worse yet, returning home without treatment.
Our Story

![]()
Dr. Johnson and his team refused to benefit from this situation and pursued not-for-profit status from day one, while earmarking excess revenues for kidney disease research and education. The team was relentless in finding funding for patients who couldn’t afford treatment. Using Kentucky Fried Chicken buckets, DCI doctors and staff collected donations at some of Nashville’s busiest intersections on weekend afternoons. These donations sustained clinic operations until the Medicare ESRD Program began paying for outpatient dialysis in 1973, and patients across the U.S. were eligible for funding to continue dialysis treatment.
Dr. Doug Johnson and Dr. H. Keith Johnson